
UBINIG/TABINAJ
Betel quid or Paan-jarda use is a common practice among men and women in the rural and urban lower income groups. This is a socially accepted practice and unlike cigeratte or biri does not have any cultural barrier. Although it is an open practice, there is gap of information about the users, which becomes a constraint in developing any regulatory framework for reducing consumption under the provision of the existing tobacco control law as amended in 2013.
So far the information available about users is from Global Adult Tobacco Survey, 20091.
In Bangladesh 43.3% of adults (41.3 million) currently use tobacco in smoking and/or smokeless form. Out of the total tobacco users 27.2% (25.9 million adults) currently (2009) use smokeless tobacco with 26.4% of men and 27.9% of women showing a higher rate among women.
Other information include
| Categories | Men | Women |
| Daily smokeless tobacco users | 20.7% | 26.6% |
| Current smokeless tobacco users, who plan to quit | 61.1% | 37.4% |
| Smokeless users advised to quit by a health care provider in past 12 months | 35.5% | 55.6% |
| Current Users | Non-current users | |
| Adults who believe smokeless tobacco use causes serious illness | 91.5% | 93.2% |
GATS, 2009
In all the categories, the indicators show trend among women with not only higher use, but also that they are not planning to quit, although they are more advised by health care providers because of serious illnesses.
Lack of awareness contributes to the low number of quit attempts for smokeless tobacco users in the Region. For example, the percentages of users who made a quit attempt in the past year was very low in Bangladesh (29%), India (35%) and Thailand (22%).
Prevalence of smokeless tobacco use among adults (current users) in the South-East Asia Region 2
———————————————
1 Global Adult Tobacco Survey (GATS) Fact Sheet, Bangladesh 2009, WHO, CDC, GOB, GTSS, MPOWER, December, 2009
2 90% of smokeless tobacco users live in South-East Asia, WHO SEARO, SEAR/PR 1563, 2013
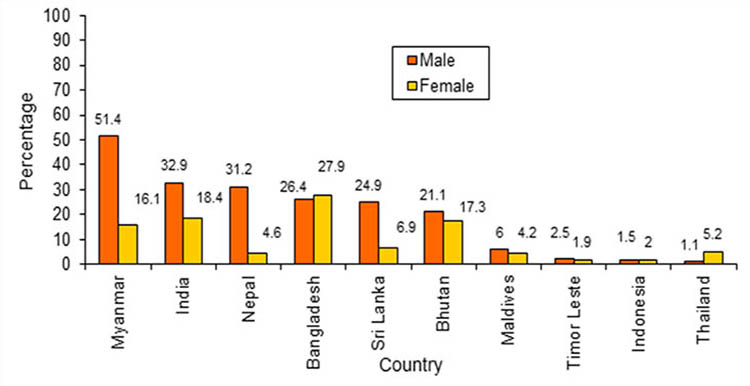
Bangladesh is the only country in the region followed by Bhutan which has higher use of smokeless tobacco among women. Thailand has very low rate of SLT use, however more among women (5.2%) than men (1.1%). It means, there has been less effort from the tobacco control advocates to work among women for reducing tobacco use, and that the law itself did not address the issues that will help reduce consumption. The need for regulation becomes even more evident for smokeless tobacco consumption for the sake of saving women from health hazards.
Smokeless tobacco (SLT) as included in the definition of Tobacco products under the “Smoking and Tobacco Products Usage (Control) Act, 2005 (amended in 2013)” includes Zarda, Sadapata and Gul as three most used products in Bangladesh. Over 10 million women consume Zarda, Sadapata and Gul without any regulations on their use. Considering the threat that smokeless tobacco use can pose to public health , it is of critical importance to identify and promote methods for reducing the use of smokeless tobacco.
Tabinaj Survey of Jarda-Sadapata users
Tabinaj members conducted a survey in 19 districts with 288 users with a questionnaire to know about some basic facts about Jarda-Sadapata use. Although members are spread over 64 districts, these 19 districts were selected randomly on the basis of members’ capacity to provide information within a week in late April, 2017. The districts are Khulna, Bagerhat, Sathkhira, Borguna, Barisal, Manikganj, Cox’sbazar, Chittagong, Noakhali, Feni, Comilla, Rangpur, Bogra, Madaripur, Chapainababganj, Mymensingh, Jamalpur, Sirajganj and Kushtia.
———————————–
3 International Agency for Research on Cancer (IARC) Smokeless tobacco and some tobacco-specific N-Nirtosamines, vol 89 of IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Vol. 89 World Health Organization International agency for Research on Cancer; Lyon, France: 2007 in Smokeless tobacco product prices and taxation in Bangladesh: Findings from the ITC survey by N Nargis, AKMG Hussain and GT Fong, 2014
All the respondents were women over the age of 40 years (74%); with 45% over 50 years. A younger group of women (25.6%) were in the age range of 25 to 40 years. They are all married. It indicates that married women at a matured age are using betel quid more than the younger women. They are mostly from low income group with Tk.2000 – Tk.5000 monthly income (28.5%) and between Tk. 5000 – Tk.10,000 (37.5%). Only 17% of the users had monthly income of Tk.10,000.
“Paan khaoya” or consumption of betel leaf with jarda and sadapata is not seen as a social nuisance or a bad manner. One can offer Paan to guests, relatives, family members except to very young children. To have a “Paan dani” – a designated pot of paan, jarda and sadapata is common in many households. Poor people find it very attractive to offer paan to any visitor, guests and relatives as they cannot offer tea, or any snacks. But at the personal level, the consumption becomes a habit and addiction.
The users (288) in the survey were found to start at an early age of less than 20 years (43%); however the majority (79.5%) started between 20 to 30 years. This means, most women started using betel quid afer marriage. About 14% started when they were over 31 years old. Very few (6%) women started over 40 years. Those who are current users they have been consuming paan with jarda/sadapata for over 20 years.
But none of the users would admit that they were consuming paan and jarda for addiction. It was a social and family practice. Only 9% started consuming on their own initiative, 47% were influenced by mother or mother-in-law as they were making paan for them. Other family members including husband, aunts, neighbours, relatives were responsible for 36% users. Through grandmothers, only 4% users started paan. Once they started it became a habit and later they cannot stop it.
But Paan, jarda, sadapata are not any home-made products. These have to be bought from the shop and one has to spend a certain amount of money to buy paan, jarda, sadapata. The survey found that 47% users spend betwen Tk.200 to Tk. 500 for paan per month, and 28.5% spend over Tk. 500. On an average the monthly expenditure on Paan is Tk.505.
There are different brands of jarda in the shop and the users spend seperately for jarda. About 46% of the users spend Tk. 50 to Tk.200 for jarda, while 24% spend Tk.200 to Tk. 500. The average spending on jarda is Tk. 185 per month. The average yearly spending on jarda per user is Tk.2,220. The 288 users in the survey are paying Tk.53,280 per month, Tk.6,39,360 per year to the company. The alternative use of the money spent on Paan-Jarda would be, according to the users, to use for the family needs, for daily food cost. They could use it for the children’s education, particularly to buy pen, note book etc.
Expenditure on Paan with Jarda-Sadapata takes a considerable share of monthly income of these low income users. With an average of Tk. 7500 monthly incme they spend about Tk.690, which is 9.2% of the income. For the 288 users the total spending on Paan and jarda-sadapata is Tk.198,720 per month and annually Tk. 2 crore 38 lakh and 1400.
According to the GATS (2009) there are 25.9 million users of smokeless tobacco, which includes three major items Jarda, sadapata and Gul. This survey only looked at only two items Jarda and sadapata that are used with paan. According to different studies, out of 27.2% smokeless tobacco users, about 24.5% use jarda and 1.8% use sadapata. From this calculation about 68,12,000 are users of Jarda and sadapata. Using the average spending of Tk.2,220 for jarda and sadapata for the 288 users in the survey, the spending at the national level on jarda and sadapata is Tk.1512 crore and 20 lakh.
Fifty different brands of Jarda were found to be used by 288 users. The brands of Jarda that are most common among these users were Hakimpuri (17%), Monipuri (7%), Shahi jarda (7%), Dhaka Jarda (7%), Baba Jarda (6%), Kanpur (4.6%) and many other small local brands . Sadapata was used by 10% of the users in the survey.
Tabinaj investigation on Price of Smokeless tobacco products:
A Tabinaj investigation of 10 retail shops among 47 retail shops in Kawran Bazar (5), Shyambazar (35) and Chawkbazar (7) was conducted during March 30-31, 2016. Fortyfive different brands of Zarda, 3 brands of Gul, 2 different sizes of Sadapata and 1 brand of Khoini were found in those shops.
Four brands of Jarda are imported from India. These are Shibdata Jarda, Nagina and Chaman Bahar opf two different size packets.
The pricing of the smokeless products are by size and amount of Jarda, Gul, Sadapata and Khoini. Only three brands of Jarda are found to be sold as piece, only Tk. 2 per piece for Mokimpuri and Golai Jarda and Tk. 5 for Dhaka Zarda.
Price range of Jarda by size and amount is the following:
7 -10 gram packater sold at Tk. 5 to Tk. 25 [brands Shantipuri, Shahi 99 Jarda and Chaman Bahar (Bangladesh)]. It may be noted that Chaman Bahar (India) is sold in 10 – 30 gram packets at Tk. 25 – Tk.60.
Five Jarda brands were found in 100 gram packs sold at Tk. 55 – Tk. 100. The brands are Surovi 55, Baba 120, Shova 55, Ratan Pati Jarda and Noorani Jarda.
The average size and amount ranges between 20 to 50 gram between the price range of Tk. 15 to 50 per packet.
The imported Jarda packets are between 10 gram to 40 gram and are sold at Tk. 25 to Tk. 75.
The prices of Jarda packs increased by Tk. 1 or 2 for low priced brands and Tk. 5 to 10 for higher brands making it less significat in terms of having an impact on the consumers.
Health effects of smokeless tobacco
- Indian experience shows that 90% cancers of oral cavity are caused by tobacco use in some form, among them more than 50% is caused by SLT.
- SLT use causes more prolonged and sustained levels of nicotine in the body than smoking.
- There is association of SLT use and CVD morbidity and mortality including myocardial infarction (heart attack), stroke and coronary artery disease.
- Risks of mycardial infarction among SLT users increased from 30% to 220% (as reported in Case Control Study in Bangladesh.
- SLT is a higher risk factor (40 – 70%) for stroke.
- SLT is associated with precancerous oral lesians; 70% of oral cancers in India are preceded by oral precancer.
- SLT use raises women’s risk of adverse reproductive outcomes.
- SLT use during pregnancy results in 70% higher anaemia, 2 – 3 times higher rate of low birth weight, 2 – 3 times higher rate of stillbirth [Source: Smokeless Tobacco and Public Health in India, Executive Summery, Ministry of Health and Family Welfare, Government of India, 2016]
- There are 49,000 oral cancer, 71,000 pharynx & larygeal cancer and 196,000 ling cancer cases in Bangladesh; out of which 3.6% of the admissions in medical college hospitals are due to cancers of oral cavity, larynx and lung.4
Tabinaj interviews of doctors on health effects of SLT
Tabinaj members interviewed doctors in 19 districts [Khulna, Bagerhat, Sathkhira, Borguna, Barisal, Manikganj, Cox’sbazar, Chittagong, Noakhali, Feni, Comilla, Rangpur, Bogra, Madaripur, Chapainababganj, Mymensingh, Jamalpur, Sirajganj and Kushtia]. They interviewed general practitioners, dentists and gynecologists.
The medical practitioners are aware of the health effects of SLT use as they were getting patients with various health problems. They have identified particular health effects due to use of smokeless tobacco as unlike smoking, smokeless tobacco goes into the blood stream and causes health hazards. It causes various problems of the gum and teeth, lesions inside the mouth, oral cancer, throat cancer, pancreas and stomach cancer. SLT users may also get liver diseases.
Pregnant women consuming SLT may deliver low weight babies, can have still birth and babies with birth defects. The brain of the baby can get affected. It can increase the threat of maternal mortality and infant mortality.